In the place of its attachment to labrum glenoidale |
Lesion, which can be connected
with a damage of labrum glenoidale in this localization, is in the foreground of
an interest. An important fact is that ruptures, which frequently affect the
tendon of the long head of the biceps in this place, are parcial, and so these
ruptures are mostly considered as tendinitis. On the other hand, probably
tenovaginitis of the long head of the biceps, which is inducted by the rupture,
are very often main causes of
patient’s problems, so it means that also targetable therapy of this
tenovaginitis (and in this case it is our belief
that a local application of steroids is suitable) can bring a big relief. With
regarding to the possibilities of present therapeutical methods the resolution
of the rupture and tenovaginitis does not become only an academic question,
but a basic condition of the right therapeutical method.
In progress of a tendon distally from an attachment
to labrum glenoidale right to muscular substance of m. biceps
brachii (approximately from bicipital groove)
|
A long head of the biceps distally from the attachment to tuberculum scapulae superglenoidalis (from the upper edge of a proximal part of the bicipital groove) is already well accessible to the ultrasound examination. In this area the diagnosis is relatively clear in the case of localization of a rupture which goes through superficial fascia. At the complete rupture the bicipital groove stays empty, and the tendon is not found during the ultrasound examination at all. This rupture is very frequent ( see following picture). We have not met a complete rupture of this type for five years of outpatient department practice.
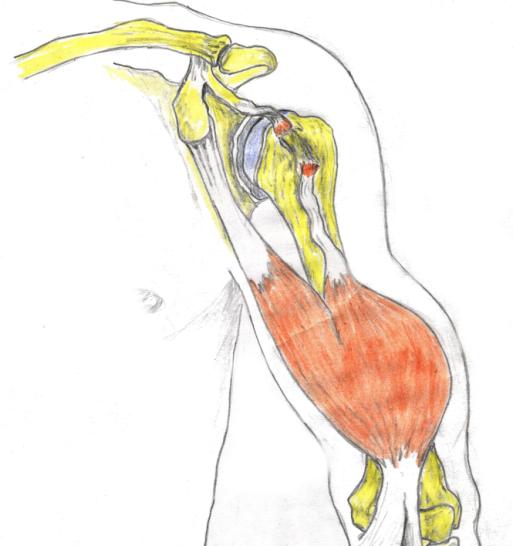
picture of a complete rupture of the long head in progress
of bicipital groove
Rupture of the Tendon of the Long Head of the Biceps in the muscle of biceps brachii
|
All the
ruptures of m. biceps brachii were found only in the place of a passage of the
tendon to the muscle, and they created a typical lump
during flexion in the elbow, and they all were mostly
parcial6.

![]()
A determination of diagnosis especially of parcial anchored
ruptures of the long head of the biceps belongs to difficult tasks in
differential diagnostics of pains in the shoulder girdle7. If there is a
suspicious that there is possible to carry out some of other examinations
(except ultrasound) of these ruptures. This examination would eventually confirm
the parcial anchored ruptures:
MRI | |
|
arthroscopy of the glenohumeral articulation |
![]()
5i. e. arthroscopic suturas labrum glenoidale
6 at the ultrasound examination there was not any empty groove of the long head of the biceps
7 injury anamnesis is a base for the suspicion of the
rupture, but unfortunately spontaneous ruptures are also very frequent
{kind=link}